ALLERGY TESTING & EVALUATION
Allergy Testing in NYC: Find the Right Test, Not Just More Tests
Published by Dr. Shilpa Paradkar Singh, MD

- Skin Testing
75+ Antigens
- Same Visit Results
Readout in 15 Minutes
- Insurance Accepted
Most Major Plans
- Midtown East
160 East 56th Street
Fast answer
Not every stuffy nose, rash, cough, stomach symptom, or episode of fatigue is an allergy. At Atrium Medical in Midtown Manhattan, we start with the pattern: when symptoms happen, where they happen, what changed, what medications you take, what you are exposed to at home or work, and what the test result would actually change. Then we test when it answers a real clinical question.
Atrium Medical offers in-office skin prick allergy testing — with results reviewed during the visit in most cases — for many common environmental and selected food allergens. We may also use blood testing when it is the better choice, especially when a patient cannot stop antihistamines, has certain skin conditions, or needs a different testing pathway.
The goal is not to hand you a huge list of things to fear. The goal is to connect your real symptoms to real triggers, then build a practical plan that fits your life in New York City.
Atrium Medical is located at 160 East 56th Street, 12th Floor, a short walk from the 59th Street subway hub and Grand Central. Same-day and next-day appointments are often available. We accept Aetna, Cigna, Blue Cross Blue Shield, UnitedHealthcare, Oxford, Medicare, and most major plans. Book online, check insurance, or call 212-457-1722.
On This Page
- When allergy testing actually helps
- Allergy symptoms versus cold, sinus, asthma, reflux, and irritants
- Skin prick testing versus blood testing
- What we commonly test for
- What a positive allergy test does and does not mean
- NYC allergy triggers: pollen, apartments, office HVAC, mold, pets, and dust
- Food allergy, food intolerance, and why IgG food sensitivity panels mislead people
- Why allergies may feel worse every year
- Emerging research: salt, inflammation, and allergic rhinitis
- What happens during an Atrium allergy testing visit
- Treatment after testing
- OTC allergy medications: what actually works
- When primary care is enough and when you need an allergist
- Insurance, location, and booking
- Allergy Testing FAQ
When allergy testing actually helps
Allergy testing is most useful when symptoms follow a pattern. A test should answer a question you and your clinician already have, not create a random list of positives that may or may not matter.
 Seasonal congestion, sneezing, itchy eyes, or post-nasal drip that returns at the same time every year.
Symptoms that get worse around pets, dust, mold, carpeting, bedding, construction dust, or a specific apartment or office.
Hives, itching, or swelling that seem tied to foods, medications, insect stings, latex, or other exposures.
Cough, wheeze, or chest tightness that may overlap with asthma or allergy-triggered airway irritation. Recurring symptoms being treated as sinus infections but returning without a clear infectious pattern.
Food reactions where the timing, dose, and symptoms suggest a possible true allergy rather than intolerance.
Seasonal congestion, sneezing, itchy eyes, or post-nasal drip that returns at the same time every year.
Symptoms that get worse around pets, dust, mold, carpeting, bedding, construction dust, or a specific apartment or office.
Hives, itching, or swelling that seem tied to foods, medications, insect stings, latex, or other exposures.
Cough, wheeze, or chest tightness that may overlap with asthma or allergy-triggered airway irritation. Recurring symptoms being treated as sinus infections but returning without a clear infectious pattern.
Food reactions where the timing, dose, and symptoms suggest a possible true allergy rather than intolerance.Testing is less useful when it is ordered as a giant panel without a clinical story. That is how patients end up with confusing reports, unnecessary food avoidance, and anxiety instead of relief.
Allergy symptoms versus cold, sinus, asthma, reflux, and irritants
This is where primary care matters. A specialist allergy clinic may focus narrowly on allergy. A primary care practice has to ask the broader question: is this actually allergy, or is something else imitating it? By evaluating allergy symptoms in a primary care setting, we can consider the broader respiratory, medication, reflux, sleep, and immune context that may be contributing.
This is also where triage matters. If symptoms are severe, sudden, or concerning for infection, an asthma flare, or another urgent problem, the practical question may be urgent care versus primary care before allergy testing.
| Possibility | Common clues |
|---|---|
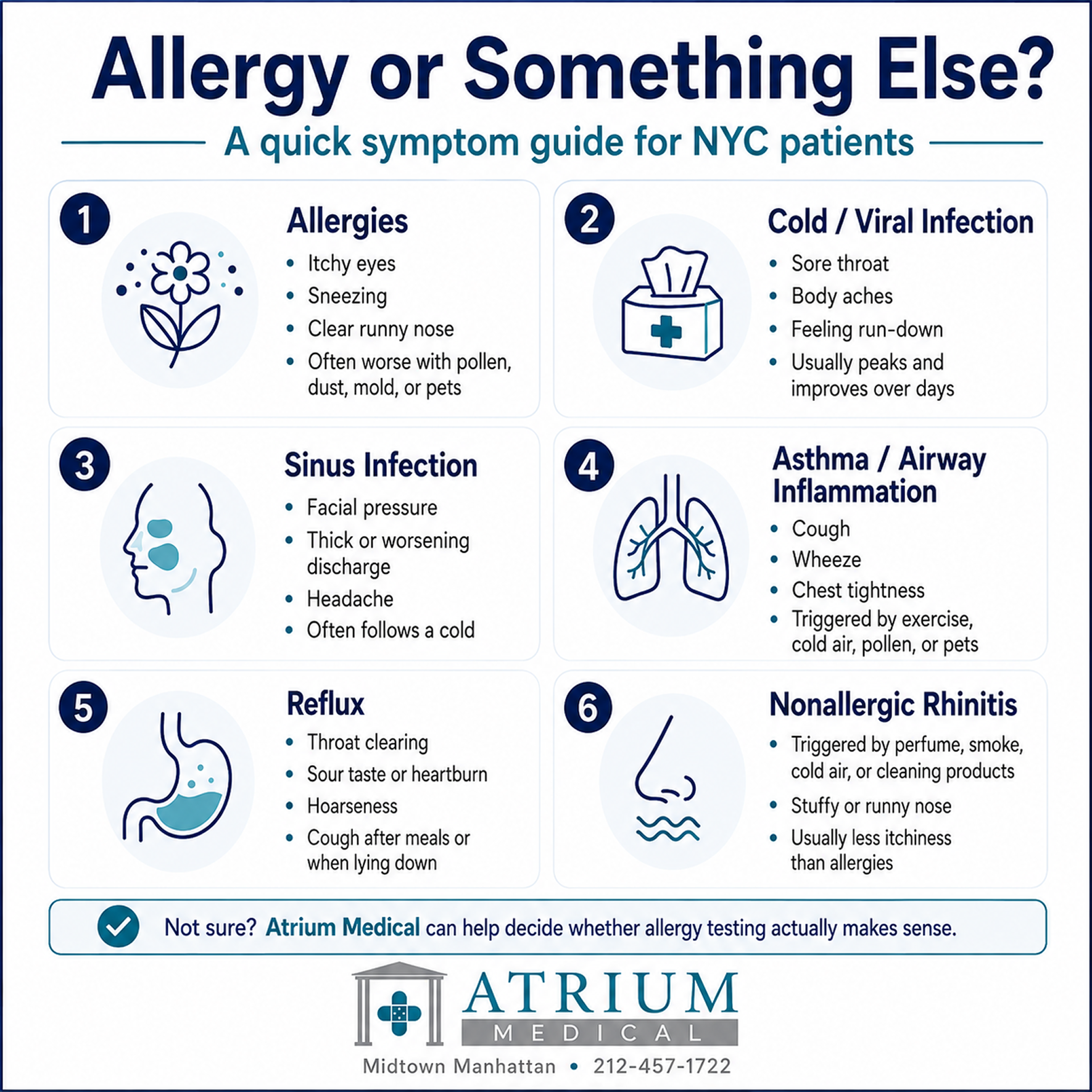
| Allergies | Itchy eyes, sneezing, clear runny nose, congestion, post-nasal drip, symptoms around pollen, dust, mold, pets, or seasonal changes. |
| Cold or viral infection | Sore throat, body aches, fever, new exposure to illness, symptoms that peak and resolve over days rather than returning in a pattern. |
| Sinus infection | Facial pressure, thick discharge, worsening after an initial viral illness, fever or one-sided symptoms in some cases. |
| Asthma or airway inflammation | Cough, wheeze, chest tightness, symptoms with exercise, cold air, pollen, dust, pets, or respiratory infections. |
| Reflux | Throat clearing, chronic cough, sour taste, hoarseness, symptoms after meals or lying down, often mistaken for post-nasal drip. |
| Nonallergic rhinitis | Congestion or runny nose triggered by cold air, perfume, smoke, cleaning products, spicy food, or weather changes without true allergic sensitization. |
| Medication effects | Dryness, congestion, cough, or rash related to new medications, supplements, nasal sprays, or overuse of decongestants. |
Skin prick testing versus blood testing
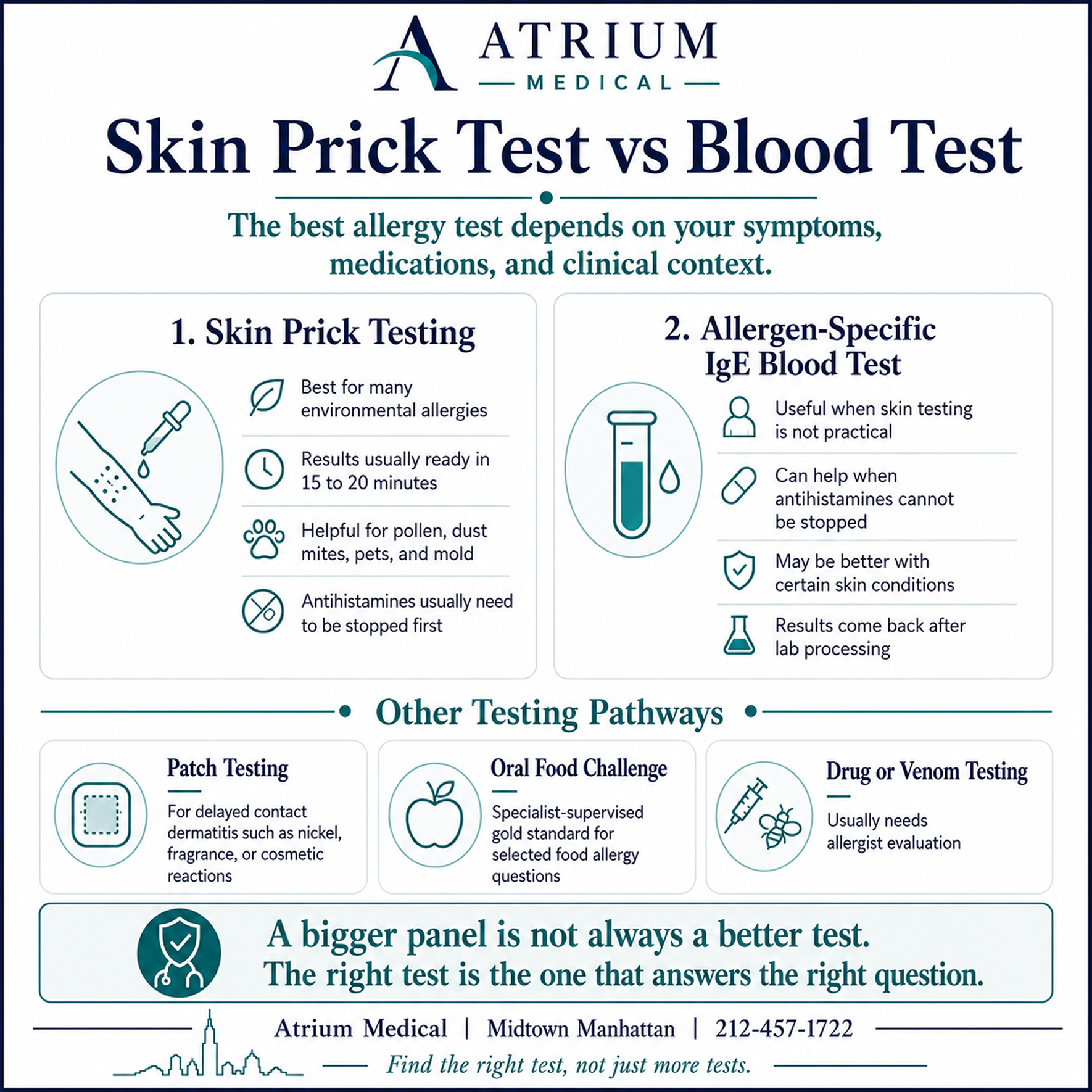
The right allergy test depends on the symptom pattern, the suspected trigger, the patient’s medications, and the risk of reaction. A test is not better because it is bigger. A test is better when it answers the right question.
| Test type | When it helps |
|---|---|
| Skin prick testing | Often best for common environmental allergies. Results are usually visible in 15 to 20 minutes. Requires avoiding antihistamines in advance. |
| Allergen-specific IgE blood testing | Useful when skin testing is not practical, when antihistamines cannot be stopped, when skin disease interferes with testing, or when a specific IgE question needs lab confirmation. |
| Patch testing | Used for delayed contact dermatitis such as reactions to nickel, fragrances, preservatives, cosmetics, or topical products. Often requires dermatology or allergy referral. |
| Oral food challenge | The supervised gold standard for many food allergy questions. This is a specialist procedure and should not be attempted at home. |
| Drug or venom allergy testing | Higher-risk testing that should generally be handled by an allergist, especially for penicillin, NSAIDs, insect stings, or prior severe reactions. |
How to prepare for skin testing
Antihistamines can suppress skin test reactions and create false negatives. Most standard antihistamines need to be stopped 5 to 7 full days before skin prick testing. This includes medications such as cetirizine, loratadine, fexofenadine, levocetirizine, diphenhydramine, and some sleep aids or cold medications that contain hidden antihistamines. Do not guess. If you take daily medications, have asthma, have a history of severe allergic reactions, or are unsure whether a medication affects testing, call Atrium before the visit.
What we commonly test for
At Atrium Medical, testing is tailored to the patient. Not everyone needs the full panel. For a Midtown office worker with spring congestion, tree pollen, grass, ragweed, dust mites, mold, and pet dander may be the most useful starting point. For a patient with mouth itching after raw apples or peaches, pollen-food cross-reactivity may be more relevant.
| Category | Examples and notes |
|---|---|
| Seasonal pollens | Tree pollen, grass pollen, ragweed, and weeds. Useful for spring, summer, and fall symptom patterns. |
| Indoor allergens | Dust mites, mold, pet dander, cockroach allergens, and other year-round triggers common in NYC apartments and offices. |
| Selected food allergens | Peanut, tree nuts, shellfish, fish, milk, egg, wheat, soy, and other foods when the history suggests a true food reaction. |
| Pollen-food cross-reactivity | Patterns such as birch pollen with raw apples, peaches, cherries, carrots, celery, almonds, or hazelnuts. |
| Skin or contact triggers | Latex, fragrances, nickel, preservatives, cosmetics, or topical products may require patch testing or referral. |
| Higher-risk categories | Drug allergy, venom allergy, anaphylaxis, severe asthma, and complex food allergy usually require allergist involvement. |
What a positive allergy test does and does not mean
A positive allergy test means your immune system recognizes that allergen. It does not automatically prove that the allergen is the cause of your symptoms. This is one of the most important points in allergy medicine, and it is where sloppy testing causes real harm.
A patient may test positive to a food they eat every week without symptoms. A patient may test positive to dust mites but actually be flaring because of a viral infection, reflux, or office irritants. A patient may test positive to cat dander and only realize after testing that chronic low-grade congestion and fatigue have become their baseline.
The test result is a clue. The history decides whether that clue matters.
NYC allergy triggers: pollen, apartments, office HVAC,
mold, pets, and dust
New York allergies are not just about pollen counts. Midtown patients live and work in a dense indoor-outdoor system: subway platforms, office HVAC, old apartment buildings, construction dust, street pollution, pets in small apartments, and seasonal pollen moving through narrow corridors of trees, parks, and buildings.
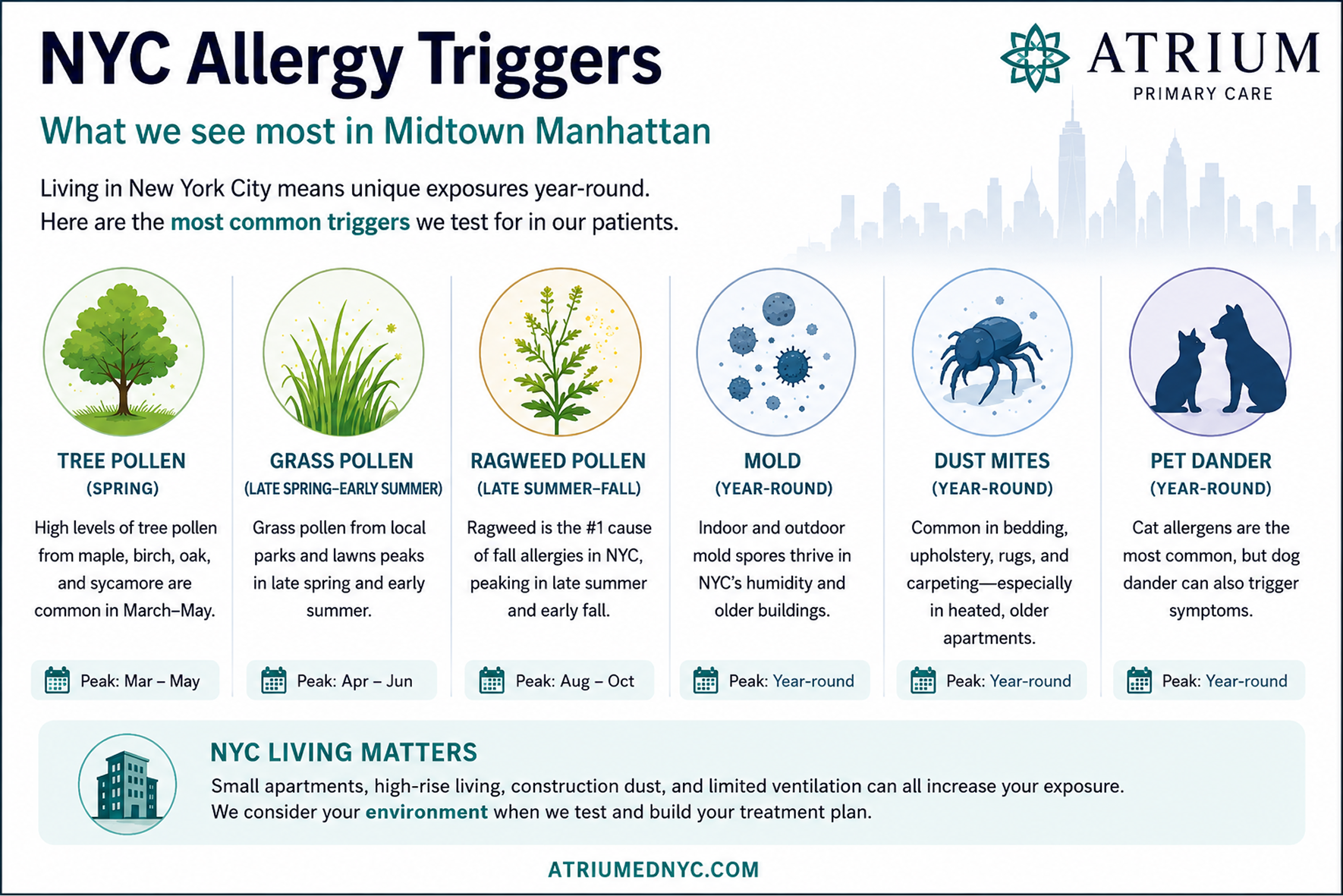
| NYC season or setting | What may be happening |
|---|---|
| February to March | Tree pollen can begin earlier than patients expect during warm spells. Some patients think they have a lingering winter cold when early pollen is already part of the picture. |
| April to June | Peak tree pollen. Oak, birch, maple, and other trees can drive congestion, sneezing, itchy eyes, and post-nasal drip. |
| May to June | Grass pollen starts as tree pollen tapers, so symptoms can feel continuous from spring into early summer. |
| July to August | Pollen may be less dominant for some patients, but mold, humidity, indoor air conditioning, and poorly maintained filters can become more relevant. |
| August to October | Ragweed season. Ragweed pollen can travel long distances, so symptoms can flare even when there is no obvious vegetation nearby. |
| Year-round | Dust mites, mold, pet dander, cockroach allergens, office HVAC, and indoor irritants do not follow a clean season. |
Knowing your trigger has a practical implication most patients miss: you can prepare before the season starts. Nasal steroid sprays — Flonase, Nasacort, Rhinocort — work best when started one to two weeks before peak exposure, not after symptoms are already severe. The anti-inflammatory effect builds over time. Starting in late March before oak and birch peak in April, or in mid-August before ragweed peaks in September, produces meaningfully better symptom control than reaching for a spray after three weeks of congestion.
The NYC Department of Health issued a March 2026 health advisory specifically telling clinicians to prepare patients weeks ahead of pollen season, noting that pollen-driven asthma emergency department visits peaked on May 1 in 2025. For patients who want to know exactly which trees are on their block and when they pollinate, the NYU Center for Urban Science and Progress maintains an interactive NYC street tree pollen map at ylurban.github.io/nyc_pollen_map — showing every street tree by species, season, and allergen severity. Climate Central’s 2026 analysis found that freeze-free seasons have lengthened in most U.S. cities since 1970, including the New York region, contributing to longer allergy seasons — which is why patients who managed allergies reasonably well for years are finding the old approach is no longer cutting it.
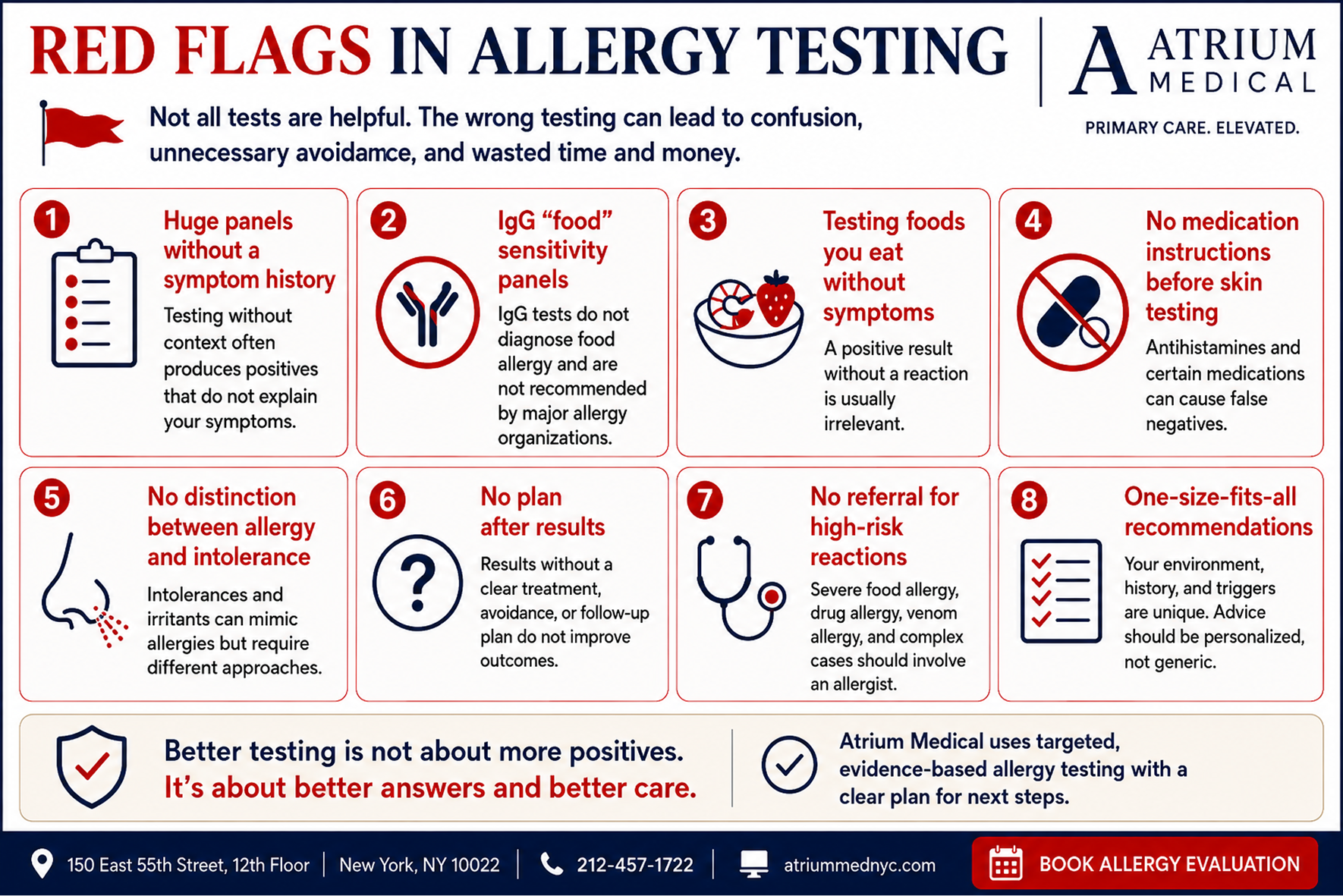
Food allergy, food intolerance, and why IgG food sensitivity panels mislead people
Food symptoms are one of the most confusing areas of allergy testing. A true food allergy is not the same as lactose intolerance, reflux, IBS, migraine triggers, celiac disease, or general food sensitivity. A true allergy usually involves an immune reaction, often IgE mediated, and may cause hives, swelling, wheezing, vomiting, throat tightness, or anaphylaxis.
Many online food sensitivity panels measure IgG antibodies. That is not the same thing as a food allergy test. Major allergy organizations warn against using IgG food panels to diagnose food allergy or food intolerance. IgG can simply reflect exposure to foods a person has eaten. Used carelessly, these panels can push patients into unnecessary restriction, fear, and nutritionally poor diets.
Atrium’s approach: start with the story, identify whether the reaction sounds allergic, decide whether IgE-based testing is appropriate, and refer to an allergist when a supervised oral food challenge or advanced workup is needed.
Oral allergy syndrome: the itchy mouth after raw fruit problem
One of the most overlooked allergy patterns is oral allergy syndrome, also called pollen-food allergy syndrome. A patient sensitized to birch pollen may develop itching or tingling in the mouth after raw apples, peaches, cherries, carrots, celery, almonds, or hazelnuts. A patient with ragweed allergy may react to melon, cucumber, zucchini, or banana. Cooking often reduces the reaction because heat changes the protein structure that the immune system recognizes. This is why testing has to be tied to a clinical pattern: the food symptom may actually be a clue to an underlying pollen allergy.
Cat allergies in New York apartments
Cat allergy is a common problem in New York because many patients live with pets in relatively small apartments with limited ventilation. The major cat allergen, Fel d 1, is lightweight, sticky, and easily airborne. It can settle into furniture, bedding, clothing, rugs, and walls. Some patients say they got used to their cat, but what really happened is that chronic congestion, mild sleep disruption, and low-grade inflammation became their new normal. Testing can clarify whether cat dander is actually part of the problem.
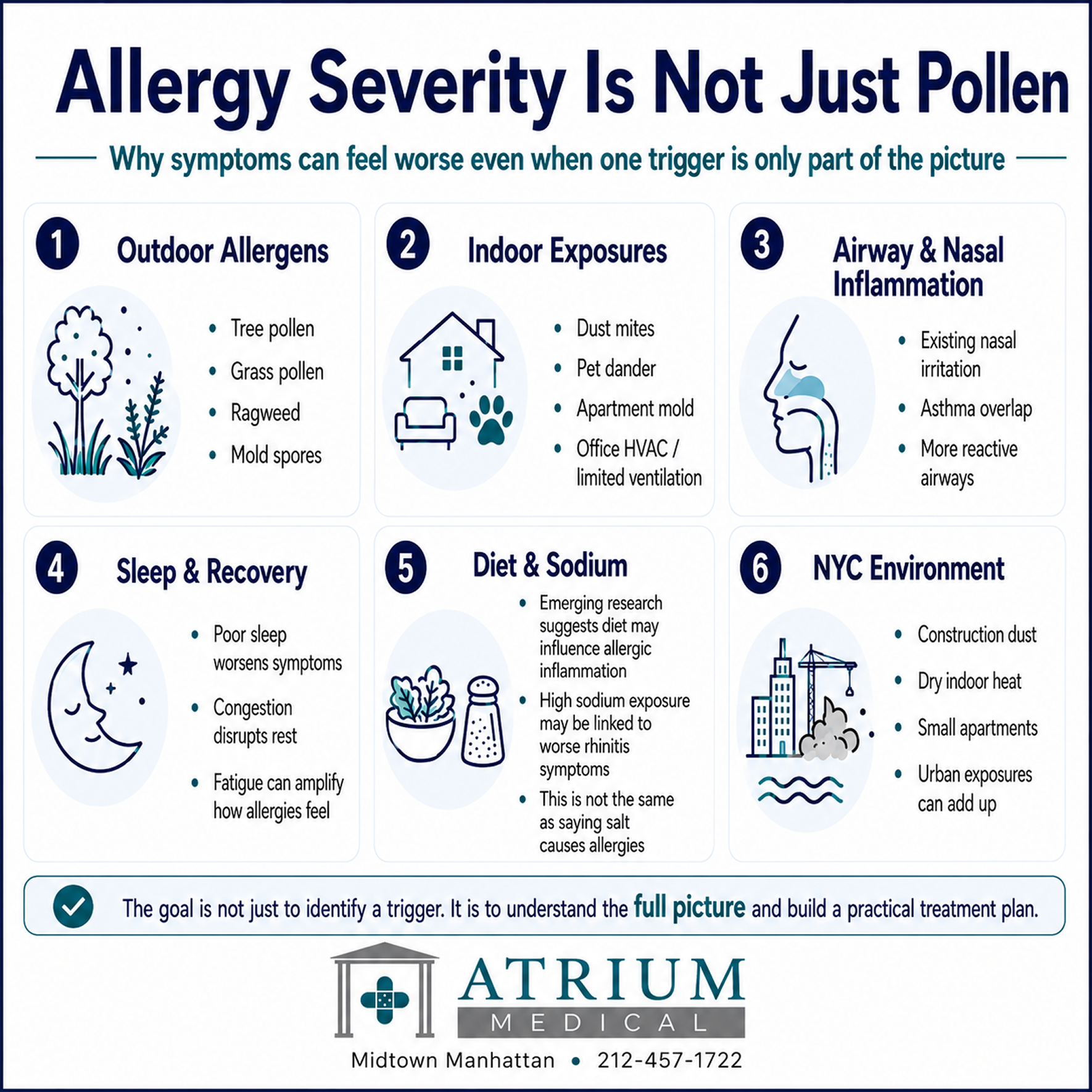
Why allergies may feel worse every year
Climate change can increase pollen concentrations and extend pollen seasons. Dense urban environments can also amplify symptoms through air pollution, construction dust, indoor air quality, mold exposure, and long hours spent inside sealed buildings.
That does not mean every patient needs more medication. It means the workup has to be smarter. The question is not only what you are allergic to. It is also when you are exposed, where symptoms happen, whether your nose and airway are already inflamed, how you sleep, what medications you take, and whether non-allergic triggers are piling on top of true allergy
Emerging research: salt, inflammation, and allergic rhinitis
Pollen, dust mites, mold, pets, genetics, and environment remain the major drivers of allergic disease. But the more interesting question is why some patients feel dramatically worse than their obvious exposures would predict.
A 2026 study in npj Science of Food examined allergic rhinitis and found that higher 24-hour urinary sodium excretion was associated with higher IgE levels and worse symptom scores in a small patient group. In mouse and cellular models, high salt exposure appeared to worsen allergic inflammation through immune signaling pathways involving NFAT5 and SGK1, with effects on the nasal mucosal barrier.
That does not mean salt causes allergies. The research is preliminary and small-sample. It means diet, inflammation, the gut microbiome, nasal barrier function, sleep, air quality, and indoor exposure may all be part of the larger picture in patients whose allergies are hard to control. Atrium discussed this research on LinkedIn as part of our broader approach to allergy care: evidence-based, current, and skeptical of simple one-factor explanations.
What happens during an Atrium allergy testing visit
Clinical history: We review symptoms, seasonality, exposures, home and office environment, pets, medications, asthma history, food reactions, and prior testing.
Test selection: We decide whether skin testing, blood testing, or referral is the right next step. Not everyone needs the same panel.
Skin prick testing when appropriate: Small amounts of selected allergens are applied to the skin with a superficial prick. Most reactions appear within 15 to 20 minutes.
Real-time interpretation: Your provider reviews what is positive, what is negative, and what actually matches your symptom pattern.
Treatment plan: We build a plan around confirmed triggers, medication timing, nasal sprays, eye drops, environmental changes, and specialist referral if needed.
Treatment after testing
The point of testing is treatment. After your results, the plan may include:
Targeted antihistamines, nasal steroid sprays, nasal antihistamine sprays, saline rinses, or eye drops.
Starting medications before your peak season instead of waiting until symptoms are already severe.
Bedroom and apartment changes for dust mites, pets, mold, and humidity.
Office and commute strategies for Midtown patients exposed to HVAC, construction dust, pollen, and irritants.
Asthma evaluation or referral if cough, wheeze, or chest tightness is part of the story.
Allergist referral for immunotherapy, complex food allergy, drug allergy, venom allergy, or high-risk reactions.OTC allergy medications: what actually works
Over-the-counter allergy medications are a reasonable first line for many patients. Understanding what each class does — and what has changed recently — helps patients use them correctly rather than stacking medications that overlap or substituting one that does not actually work.
Antihistamines
First-generation antihistamines — Benadryl (diphenhydramine) and similar older medications — cross the blood-brain barrier and cause drowsiness, impaired driving, and cognitive effects. They are not appropriate for regular daily use. Second-generation antihistamines — cetirizine (Zyrtec), loratadine (Claritin), fexofenadine (Allegra), and levocetirizine (Xyzal) — are the better choice for ongoing allergy management. They work within a few hours and can be taken daily. Of these, fexofenadine is the least sedating. Cetirizine can cause mild drowsiness in some patients even though it is classified as second-generation.
Important for testing: all antihistamines must be stopped 5 to 7 full days before skin prick testing. Many sleep aids, cold medications, and stomach medications contain hidden antihistamines — check labels or call before the visit.
Nasal steroid sprays
Nasal steroid sprays — Flonase (fluticasone), Nasacort (triamcinolone), Rhinocort (budesonide) — are the preferred daily treatment for allergic rhinitis according to most allergy guidelines. They reduce nasal inflammation directly, can be appropriate for daily use, and are available in age-appropriate formulations for children. The key point most patients miss: they take a few days to two weeks to reach full effect. They are not rescue medications. Starting one to two weeks before your known trigger season produces substantially better results than waiting until you are already symptomatic.
Decongestants: what changed and what still works
This is where patients need to know something important. There are effectively two different products sold under the Sudafed brand name, and only one of them works.
Original Sudafed contains pseudoephedrine, a highly effective oral decongestant. Because pseudoephedrine can be used to manufacture methamphetamine, Congress moved it behind the pharmacy counter in 2006 (Combat Methamphetamine Epidemic Act). It is still available — you just need to ask the pharmacist and show ID.
Sudafed PE and many reformulated cold products on open shelves contain oral phenylephrine instead. An FDA advisory panel voted 16 to 0 in September 2023 that oral phenylephrine is no more effective than a placebo as a nasal decongestant — it is metabolized so rapidly in the gut and liver that almost none reaches the bloodstream. The FDA formally proposed removing oral phenylephrine from its approved OTC list in November 2024. Many retailers have already pulled single-ingredient oral phenylephrine products.
One important distinction: the FDA’s proposal applies only to oral phenylephrine pills and liquids, not nasal sprays. Nasal decongestant sprays such as oxymetazoline (Afrin) and phenylephrine (Neo-Synephrine) bypass the digestive tract and act directly on nasal tissue. They can work quickly, but they should generally not be used for more than three consecutive days because of rebound congestion (rhinitis medicamentosa).
Bottom line on decongestants: if you want an oral decongestant that works, ask the pharmacist for the original pseudoephedrine-based Sudafed from behind the counter. If you need short-term nasal congestion relief, a nasal spray decongestant works but limit use to three days. Sudafed PE and similar oral phenylephrine products on the open shelf are likely ineffective for congestion.
When primary care is enough and when you need an allergist
| Often reasonable to start with Atrium primary care | Usually needs allergist or urgent care pathway |
|---|---|
| Seasonal congestion, sneezing, itchy eyes, and post-nasal drip. | Anaphylaxis, throat tightness, fainting, or severe swelling. |
| Mild hives without breathing symptoms or swelling. | Severe asthma, wheezing, or shortness of breath. |
| Suspected dust, mold, pet, pollen, or apartment triggers. | Drug allergy testing or venom allergy testing. |
| Medication review for allergies that are not responding. | Complex food allergy or need for oral food challenge. |
| Initial food reaction assessment when the history is not high risk. | Immunotherapy or allergy shots. |
| Allergy testing to guide treatment timing and environmental changes. | Recurrent severe reactions without a clear trigger. |
If you are having trouble breathing, throat tightness, severe swelling, fainting, or symptoms of anaphylaxis, call 911 or seek emergency care immediately.
Insurance, location, and booking
Atrium Medical is located at 160 East 56th Street, 12th Floor, in Midtown East, a short walk from the 59th Street subway hub and convenient to Park Avenue, Lexington Avenue, Third Avenue, Sutton Place, Turtle Bay, Grand Central, and the broader Midtown office corridor.
We accept Aetna, Cigna, Blue Cross Blue Shield, UnitedHealthcare, Oxford, Medicare, and most major commercial insurance plans. Allergy testing is often covered when medically necessary, but coverage depends on the plan, deductible, copay, diagnosis, and type of test ordered. Our team can help verify benefits before your visit.
To schedule an allergy evaluation, book online or call 212-457-1722. Same-day and next-day appointments are often available. New patients can also review what to expect at a new patient visit before scheduling.
Allergy Testing FAQ
You may benefit from allergy testing if your symptoms are recurrent, seasonal, exposure-related, or not responding to routine treatment. Testing is especially useful when the result will change the treatment plan: medication timing, avoidance strategy, food decision, pet exposure plan, or referral decision.
Sometimes, yes. If symptoms are mild, clearly seasonal, and controlled with over-the-counter medication, testing may not be necessary. Testing becomes more useful when symptoms are persistent, severe, confusing, year-round, or linked to foods, pets, mold, dust, or work or home exposure.
Most reactions appear within 15 to 20 minutes. Your provider can usually review results during the same visit.
Skin prick testing is usually more like a light scratch than a shot. If you react to an allergen, the spot may itch briefly and form a small bump similar to a mosquito bite.
Yes. Antihistamines can block skin reactions and cause false negatives. Most standard antihistamines should be stopped 5 to 7 full days before skin prick testing. Call us before the visit if you take allergy medicine, cold medicine, sleep aids, stomach medicine, psychiatric medication, or any medication you are unsure about. Do not stop important medications without guidance.
For many environmental allergies, skin testing is fast and clinically useful because results are visible during the appointment. Blood testing is helpful when skin testing is not practical, when medications cannot be stopped, or when a specific IgE question needs lab confirmation.
Skin testing and IgE blood testing can help evaluate possible food allergy, but results must be tied to the history. A positive food test alone is not a diagnosis. If the situation is high risk or unclear, an allergist may be needed for supervised testing or oral food challenge.
Food allergy involves the immune system and can cause hives, swelling, wheezing, vomiting, throat tightness, or anaphylaxis. Food intolerance is different and may involve digestion, enzyme deficiency, reflux, IBS, dose, or sensitivity to certain ingredients.
Many online food sensitivity tests use IgG panels. Major allergy organizations do not recommend IgG testing to diagnose food allergy or food intolerance. These tests can produce confusing results and unnecessary dietary restriction.
Yes, indirectly. Allergies can worsen sleep, nasal obstruction, sinus pressure, and daytime fatigue. But fatigue and brain fog have many causes, so persistent symptoms deserve a broader primary care evaluation.
Yes. Allergies and colds can both cause congestion, runny nose, sneezing, cough, and throat irritation. Itchy eyes, a recurring seasonal pattern, and symptoms around triggers point more toward allergy. Fever, body aches, and a short course that resolves over days point more toward infection.
Yes. Post-nasal drip and allergic airway irritation can cause cough. But cough can also come from asthma, reflux, infection, medication effects, or lung disease. If cough is persistent, recurrent, or associated with wheeze or shortness of breath, it should be evaluated.
Older buildings, dust mites, mold after leaks, cockroach allergens, pet dander, carpeting, dry indoor air, radiators, and limited ventilation can all worsen allergy-like symptoms. Testing can help separate true allergy from irritant exposure.
Yes. Poorly maintained filters, dry air, dust, mold, and recirculated indoor allergens can worsen symptoms. Midtown patients often notice that symptoms differ between home, office, subway, and outdoors.
Adult-onset allergies are common. New exposures, moving apartments, getting a pet, workplace changes, viral illnesses, changes in immune sensitivity, and longer or more intense pollen seasons can all bring symptoms to the surface.
Sometimes the medication is not the issue. The trigger may be stronger, the timing may be wrong, nasal inflammation may need a different treatment, or the symptoms may not be allergic. Testing and clinical review can help avoid simply stacking more medications.
Yes. Allergic inflammation can block nasal drainage and create sinus pressure. But repeated sinus infections may also reflect uncontrolled allergies, nonallergic rhinitis, anatomy, reflux, or other conditions.
Yes. Nasal congestion, post-nasal drip, mouth breathing, and coughing can fragment sleep. Patients may notice fatigue before they realize allergies are part of the problem.
Yes, cat dander is commonly included when clinically appropriate. Cat allergen can persist in apartments and on fabrics and can cause chronic congestion, itchy eyes, cough, or asthma-like symptoms in sensitized patients.
That is common. The goal is not always total avoidance. For dust mites, pollen, pets, or mold, the plan may involve exposure reduction, medication timing, nasal sprays, air filtration, cleaning strategies, or allergist referral for immunotherapy discussion.
You should see an allergist for anaphylaxis, severe asthma, complex food allergy, drug allergy, venom allergy, immunotherapy, oral food challenge, or unclear high-risk reactions. Atrium can help identify when referral is the right move.
Many plans cover medically necessary allergy testing, but coverage depends on the plan, diagnosis, deductible, copay, and type of test. Atrium can help verify coverage before your visit.
Same-day and next-day appointments are often available. Call 212-457-1722 or book online.
Medical sources and official references
This page was written and reviewed by Atrium Medical Primary Care using current official guidance, clinical literature, and government sources where applicable. Sources may be updated as guidelines change.
- ACAAI: allergy testing and diagnosis overview
- AAAAI: IgG food sensitivity test position statement
- CDC: climate and pollen health effects
- CDC: climate change and allergens
- npj Science of Food: sodium intake and allergic rhinitis study 2026
- ACAAI: skin prick and blood testing overview
- AAAAI: food allergy overview and evaluation
- NYC Health Department: prepare people with asthma for pollen season (March 2026 advisory)
- NYC street tree pollen map (NYU CUSP)
- Climate Central: warmer growing season and longer allergy season 2026
- FDA: proposed order to remove oral phenylephrine from OTC monograph
Book Your Allergy Evaluation at Atrium Medical
Most allergy symptoms in New York City are treatable once the trigger is correctly identified. The first step is knowing which part of the city’s environment — pollen, apartment, office, commute, or something else — is driving them.
Atrium Medical is located at 160 East 56th Street, 12th Floor, in Midtown East Manhattan, convenient to the 59th Street subway hub, Grand Central, Park Avenue, and Lexington Avenue. Book your allergy evaluation online or call 212-457-1722.





