MEDICAL WEIGHT LOSS CARE
GLP-1 Weight Loss in NYC: Medical Supervision, Labs, Insurance, and Long-Term Follow-Up
Published by Dr. Shilpa Paradkar Singh, MD | Last reviewed June 2026

- Physician-Led Care
Continuous monitoring by NYC
experts to ensure safety and clinical
efficacy.
- GLP-1 & Oral Options
Access to the latest FDA-approved medications tailored to your biology.
- Insurance Guidance
Comprehensive navigation of prior authorizations for commercial plans.
- Long-Term Follow-Up
Maintenance strategies designed for lasting health beyond the weight loss phase.
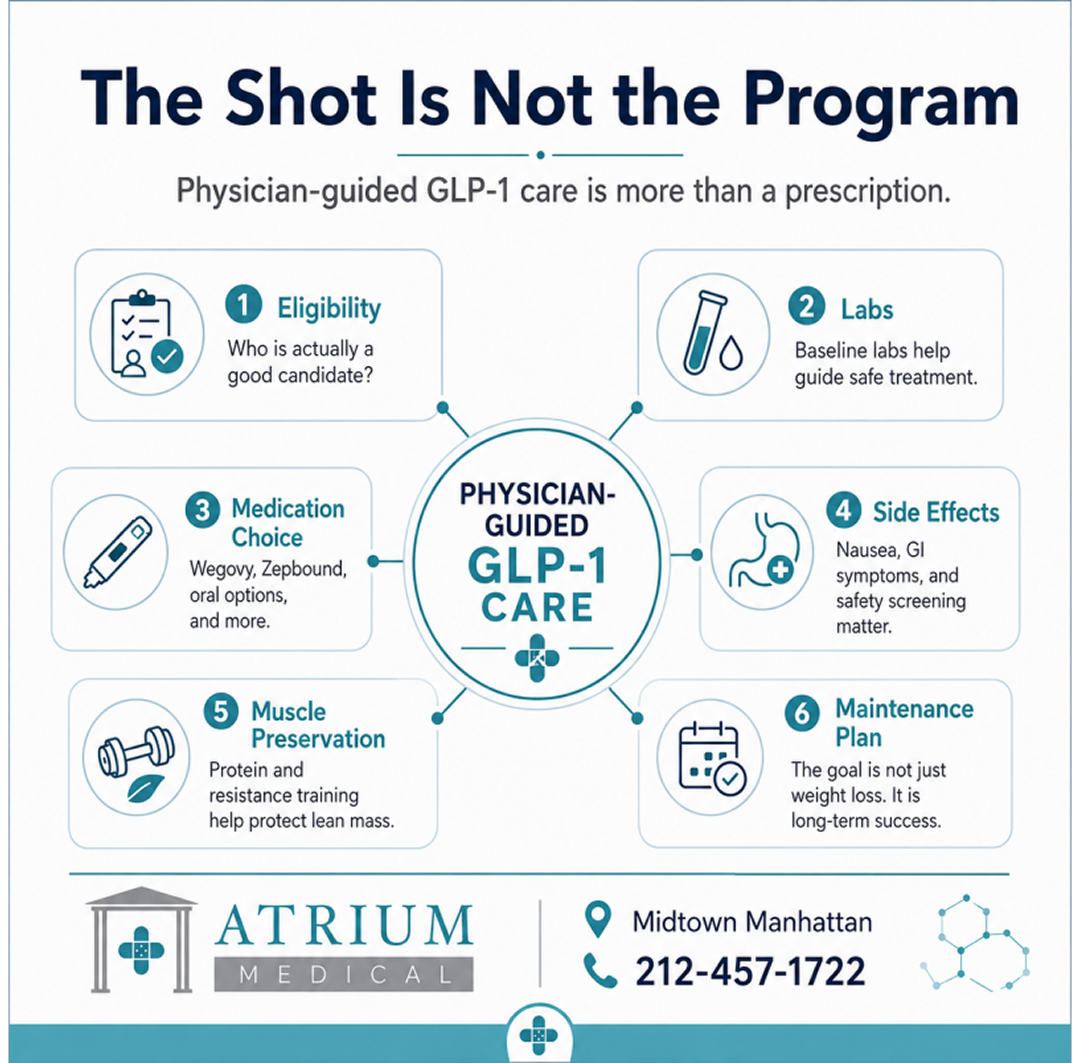
GLP-1 medications have changed obesity medicine. They have also created a noisy market of med spas, online prescribing mills, influencer claims, compounded medication confusion, and patients wondering what is medically real. At Atrium Medical in Midtown Manhattan, we take a different approach: physician-led medical weight loss inside a real primary-care practice.
We help patients decide whether medications like Wegovy, Zepbound, Ozempic, Mounjaro, Oral Wegovy, or Foundayo make sense for them, and we help patients understand emerging next-generation options such as retatrutide without confusing investigational data with an available prescription. We review the medical history, baseline labs, weight-related conditions, medication risks, side effects, insurance barriers, muscle preservation, and the long-term maintenance plan. The goal is not just losing weight. The goal is building a plan patients can actually stay on.
Weight loss is not only about the number on the scale. It is about blood pressure, blood sugar, cholesterol, fatty liver, sleep apnea, mobility, cardiovascular risk, and quality of life. That is why this belongs in primary care, not in a one-click prescription funnel.
Atrium Medical is located at 160 East 56th Street, 12th Floor, near the 59th Street subway hub and Grand Central. We offer in-person visits for evaluation, labs, vitals, side-effect assessment, and follow-up, with televisits in NYC when appropriate. To schedule a medical weight loss visit, book online, check insurance, or call 212-457-1722.
On This Page
- What medical weight loss means at Atrium
- Who is actually a good candidate?
- GLP-1 medications compared
- Injectables versus oral GLP-1 options
- Retatrutide and next-generation triple agonists
- What results are realistic?
- Side effects and safety screening
- Muscle preservation: the part people ignore
- Weight loss versus metabolic health
- Beyond weight loss: emerging organ-system benefits
- What happens after weight loss: maintenance strategy
- Insurance, prior authorization, and the 2026 Medicare GLP-1 Bridge Program
- Compounded GLP-1s and online medication risk
- PMOS, menopause, fatty liver, sleep apnea, and cardiometabolic risk
- GLP-1 microdosing and dose manipulation
- Ozempic face: Is it real?
- Buying GLP-1 medications online: what patients should know
- How Atrium manages GLP-1 care in Midtown Manhattan
- Medical Weight Loss FAQ
What medical weight loss means at Atrium
Medical weight loss is not a syringe and a slogan. It is the medical evaluation and long-term management of obesity, overweight, insulin resistance, and weight-related health risk.
At Atrium, that means we do not start with a medication menu. We start with the patient: weight history, prior attempts, family history, blood pressure, glucose, cholesterol, liver markers, sleep, medications, mental health, alcohol use, menopause or PMOS context when relevant, and what the patient is actually trying to accomplish.
For some patients, a GLP-1 or related medication may be appropriate. For others, the safer first step may be labs, lifestyle counseling, treatment of sleep apnea, medication review, or addressing a medical driver of weight gain. The point is not to be anti-medication. The point is to use medication intelligently.
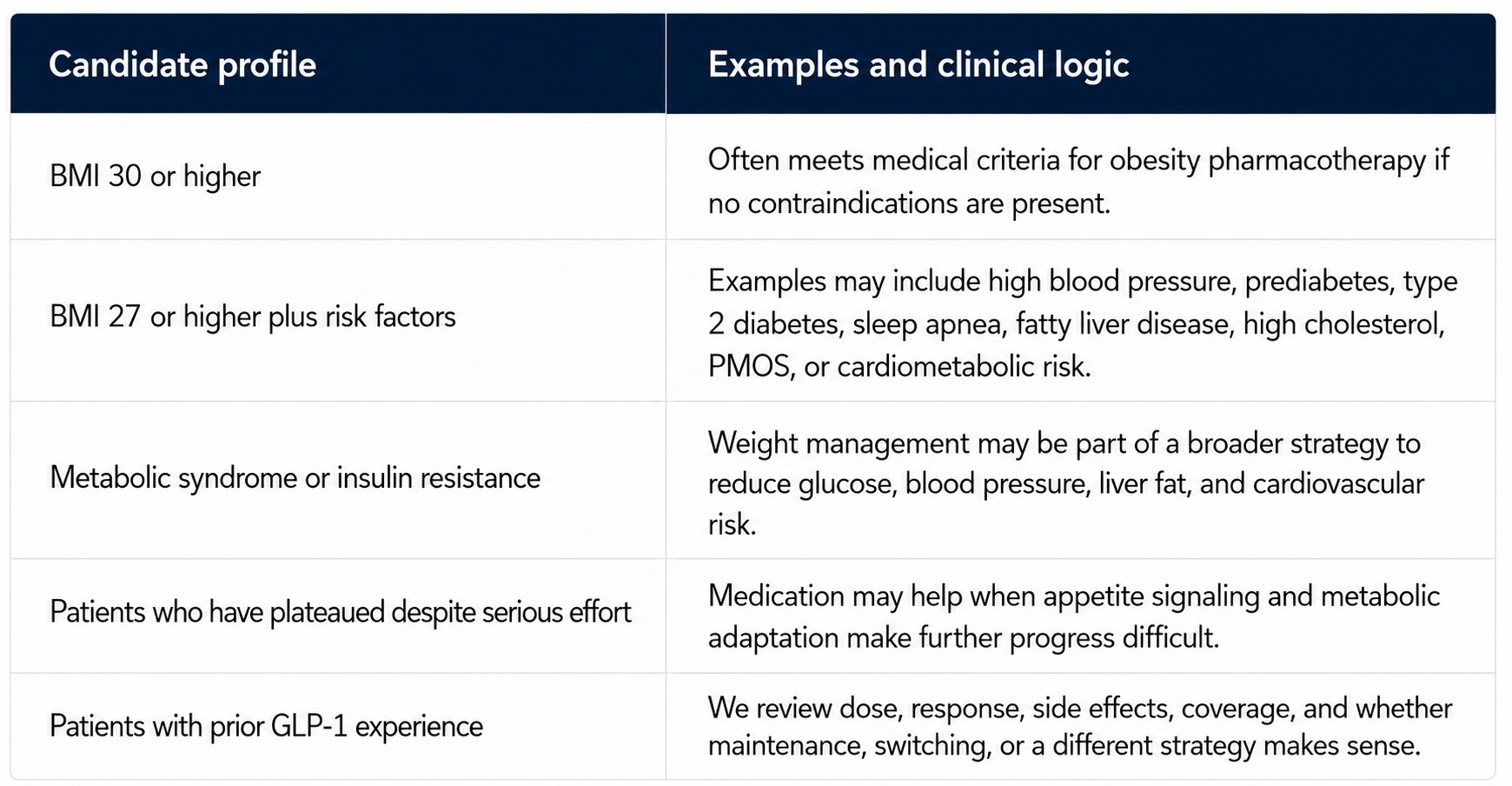
Who is actually a good candidate?
A good medical weight loss visit starts with eligibility and safety. GLP-1 and related medications are usually considered for patients with obesity or overweight plus weight-related medical conditions. They are not meant for purely cosmetic use or short-term crash dieting.
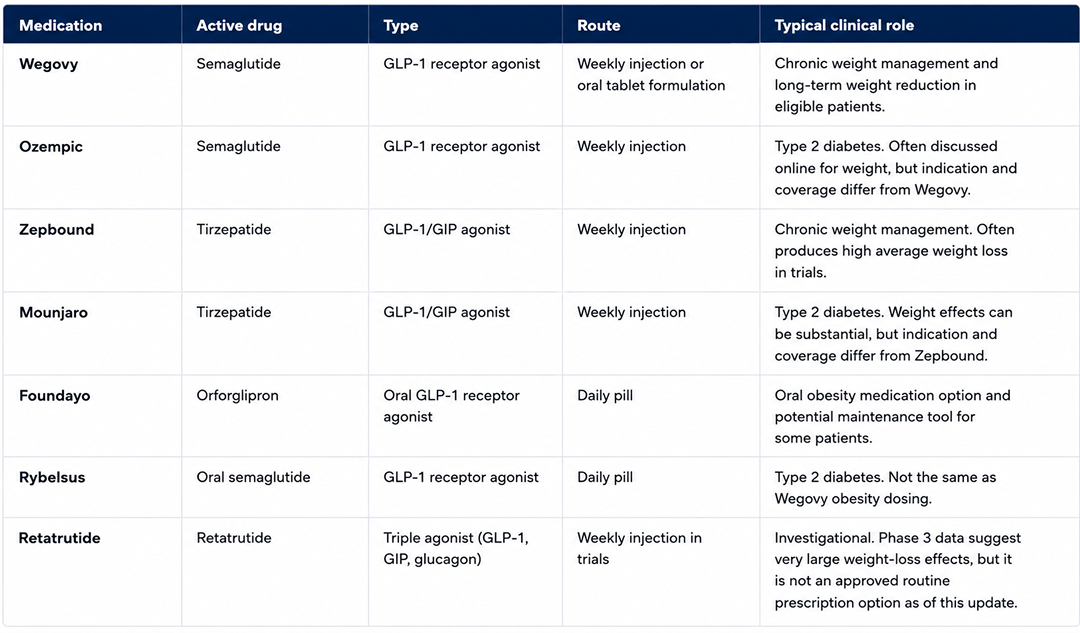
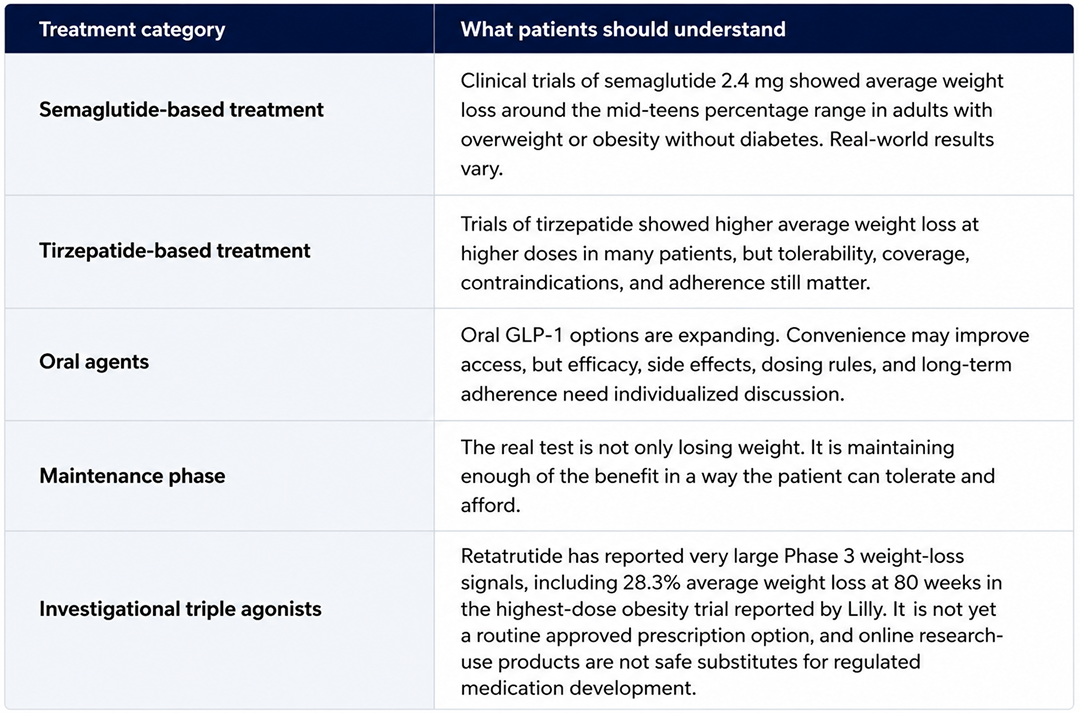
GLP-1 medications compared
Patients often hear the brand names before they understand the differences. The same active drug may appear under different brand names, with different FDA indications, doses, routes, and insurance rules.

Injectables versus oral GLP-1 options
The GLP-1 landscape is evolving quickly. For years, the most powerful weight loss medications were weekly injections. Oral options are now becoming more important, including oral semaglutide formulations and orforglipron, marketed as Foundayo.
This matters because injections are a barrier for some patients. A daily pill may be easier to start, easier to maintain, or easier to use during travel. But oral medication does not remove the need for medical supervision. Side effects, contraindications, medication interactions, insurance rules, and long-term maintenance still matter.
The right question is not “shot or pill?” The right question is: which medication is safe, effective, affordable, tolerable, and realistic for this patient to stay on?
Retatrutide and next-generation triple agonists
Retatrutide is one of the most important next-generation obesity drugs to watch. It is not simply another GLP-1. It is a once-weekly investigational triple agonist designed to activate three metabolic receptor pathways at the same time: GLP-1, GIP, and glucagon.
That matters because obesity medicine is moving beyond simple appetite suppression. GLP-1 signaling affects appetite and glucose regulation. GIP signaling may add metabolic effects. Glucagon signaling may influence energy expenditure and liver-related metabolism. The promise of retatrutide is that a single molecule may coordinate several pathways at once.
In May 2026, Lilly reported that in a late-stage trial of adults with obesity or overweight and at least one weight-related comorbidity, the highest 12 mg dose of retatrutide produced 28.3% average weight loss over 80 weeks, and more than 45% of participants lost 30% or more of their body weight. Lilly has also reported Phase 3 diabetes data showing A1C reduction and weight loss in adults with type 2 diabetes. Those signals are clinically significant, but retatrutide remains investigational and is not a routine prescription option outside clinical trials.
The practical takeaway for patients is not to look for gray-market retatrutide online. It is to understand where the field is going. The next wave of obesity medicine may include stronger, more complex metabolic therapies. That makes physician supervision, side-effect monitoring, medication legitimacy, muscle preservation, and long-term maintenance even more important.
What results are realistic?
Trial results vary by drug, dose, baseline weight, adherence, side-effect tolerance, and whether patients can stay on treatment. Many patients lose meaningful weight. Some lose less. Some stop because of side effects, coverage, cost, or life circumstances. New retatrutide data raise the ceiling for what next-generation metabolic drugs may eventually achieve, but investigational results should not be confused with an available treatment plan.
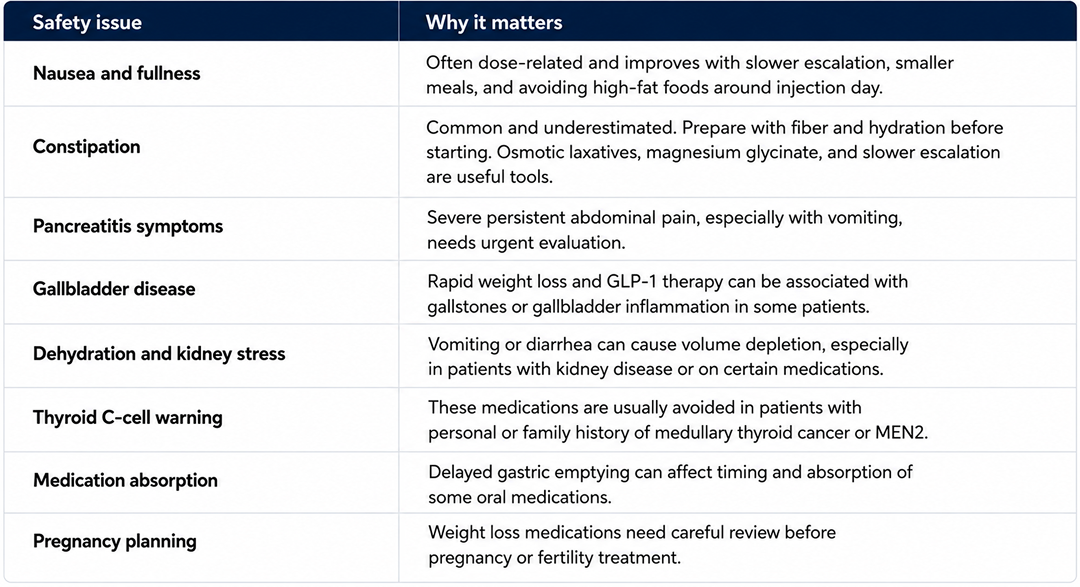
Side effects and safety screening
The most common side effects are gastrointestinal: nausea, fullness, constipation, diarrhea, reflux, and reduced appetite. These are often dose-related and may improve with slower dose escalation, hydration, fiber, protein planning, and individualized adjustments. In practice, GI side effects — especially constipation — are among the most common reasons patients struggle to stay on these medications. They are also among the most preventable with the right preparation.
Constipation: the side effect patients underestimate.
In our practice, constipation is one of the most consistently reported problems on GLP-1 therapy, particularly in the first weeks of a new dose. The likely mechanism is that GLP-1 receptor agonists slow gastric emptying and reduce peristalsis — the rhythmic muscular contractions that move stool through the colon. The result is slower transit, harder stool, and a patient who did not expect this to be part of the experience.
The most important thing to know: prepare before you start, not after the problem begins.
Before starting or escalating a GLP-1 dose, prioritize fiber and hydration. Aim for 25 to 35 grams of fiber daily from food or supplementation — psyllium husk is inexpensive and effective — and increase water intake meaningfully, not incrementally. Patients who arrive at a new dose already well-hydrated and fiber-sufficient handle the transition significantly better than those who try to adjust after constipation has set in.
If constipation becomes a problem despite preparation, options worth discussing with your clinician include:
A gentle osmotic laxative such as polyethylene glycol (MiraLAX) used on a scheduled rather than as-needed basis during dose escalation periods.
Magnesium glycinate supplementation. Magnesium has a mild stool-softening effect and is generally well-tolerated. Some patients find 200 to 400 mg at bedtime helps with both bowel regularity and sleep. This is not a prescription medication but should be discussed if you take other medications.
Metformin. Some patients are prescribed metformin as an adjunct to GLP-1 therapy for metabolic reasons — insulin resistance, prediabetes, or PMOS. Metformin has a known GI effect that tends toward looser stools in some patients, which can partially offset GLP-1-related constipation. This is not a reason to start metformin on its own, but it is a relevant consideration if metformin is already part of the clinical conversation.
Slower dose escalation. Constipation and other GI side effects are consistently worse when doses are escalated quickly. There is no rule that requires advancing on the fastest possible schedule. Staying at a lower dose longer is a legitimate clinical strategy and often produces better tolerability with only modest reduction in weight loss speed.
Muscle preservation: the part people ignore
GLP-1s reduce appetite. That is part of why they work. But if appetite falls and protein intake collapses, patients lose muscle along with fat. In some trial data, lean mass loss has exceeded what clinicians expected at higher doses and faster weight loss rates. That is not the goal.
A serious medical weight loss plan addresses muscle directly:
Protein intake. Current evidence supports 1.2 to 1.6 grams of protein per kilogram of body weight daily to preserve lean mass during caloric deficit. For a 180-pound patient, that is roughly 100 to 130 grams of protein per day — more than most patients are eating when appetite is suppressed. This does not happen by accident. It requires deliberate planning.
Resistance training. Not optional. Resistance exercise is the most effective tool for preserving lean mass during weight loss. Cardio burns calories. Resistance training signals the body to hold onto muscle. Patients on GLP-1s who are not doing any resistance training are losing more muscle than they need to.
Body composition monitoring. The scale does not distinguish between fat loss and muscle loss. Patients who want to track lean mass separately from total weight can discuss DEXA scanning or clinical body composition assessment. Not every patient needs this, but for patients with significant muscle mass concerns — older adults, perimenopausal women, patients losing weight quickly at high doses — it is worth considering.
Older adults and perimenopause. Muscle preservation is not equally important for everyone. It is most critical for patients over 50, perimenopausal or postmenopausal women, and anyone with prior sarcopenia or low baseline muscle mass. For these patients, a GLP-1 that produces large rapid weight loss without a muscle preservation strategy is trading one metabolic problem for another.
The goal is not becoming smaller at any cost. The goal is better metabolic health, better function, and a body that can sustain the result.
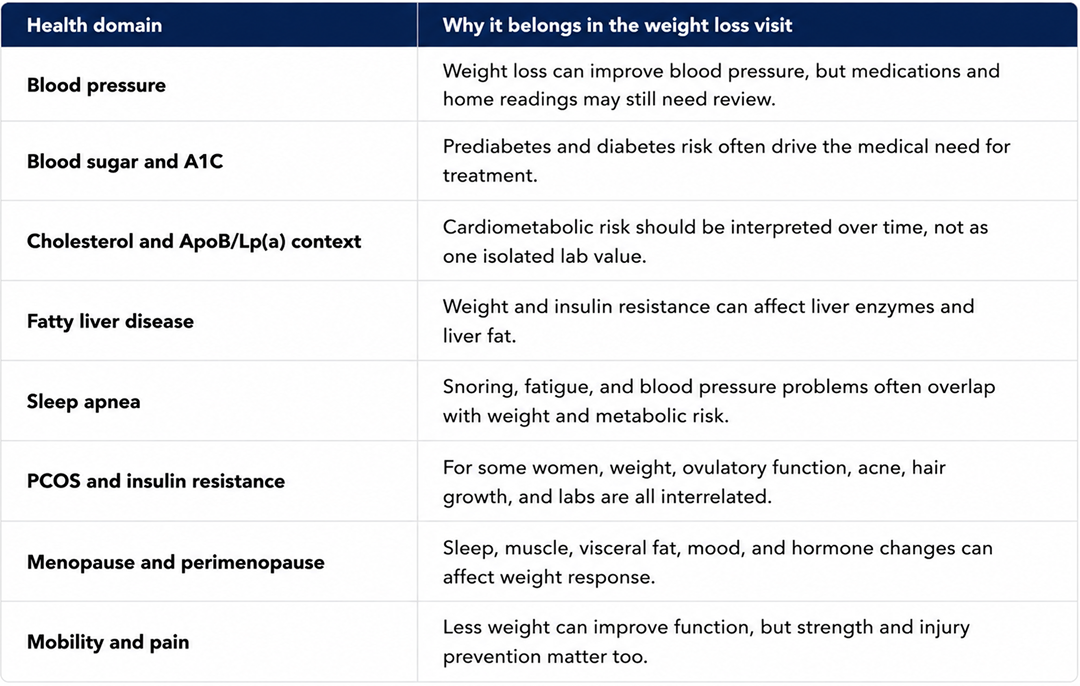
Weight loss versus metabolic health
The scale is only one marker. A patient can lose weight and still need work on blood pressure, cholesterol, fatty liver, sleep, alcohol use, or muscle. Another patient may lose a modest amount of weight but have a major improvement in blood pressure, A1C, mobility, or sleep apnea symptoms. The medical goal is bigger than a number.

Beyond weight loss: emerging organ-system benefits
A growing body of research suggests that GLP-1 medications may do more than suppress appetite and reduce weight. In several organ systems, at least part of the benefit appears to occur before major weight loss or independent of the number on the scale. That does not mean every result is proven for every patient. It does mean the science is moving toward a broader view of GLP-1s as metabolic regulators, not just obesity drugs.
For patients and clinicians, this matters because it changes how we think about outcomes. A good GLP-1 visit is not only about pounds lost. It is also about blood pressure, inflammation, kidney protection, fatty liver disease, cardiovascular risk, sleep, mobility, and overall metabolic health.
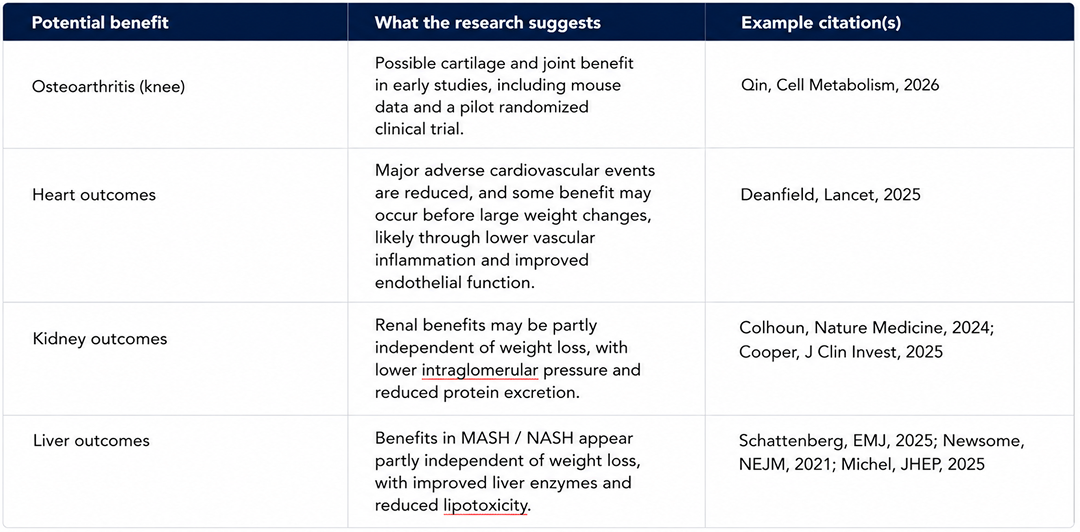
These data are promising, but they should not be oversold. Some outcomes are already supported by large trials. Others remain emerging or indirect. The point is not that GLP-1s are magic. The point is that they appear to be systemic metabolic therapies with effects that reach beyond simple appetite suppression.
What happens after weight loss: maintenance strategy
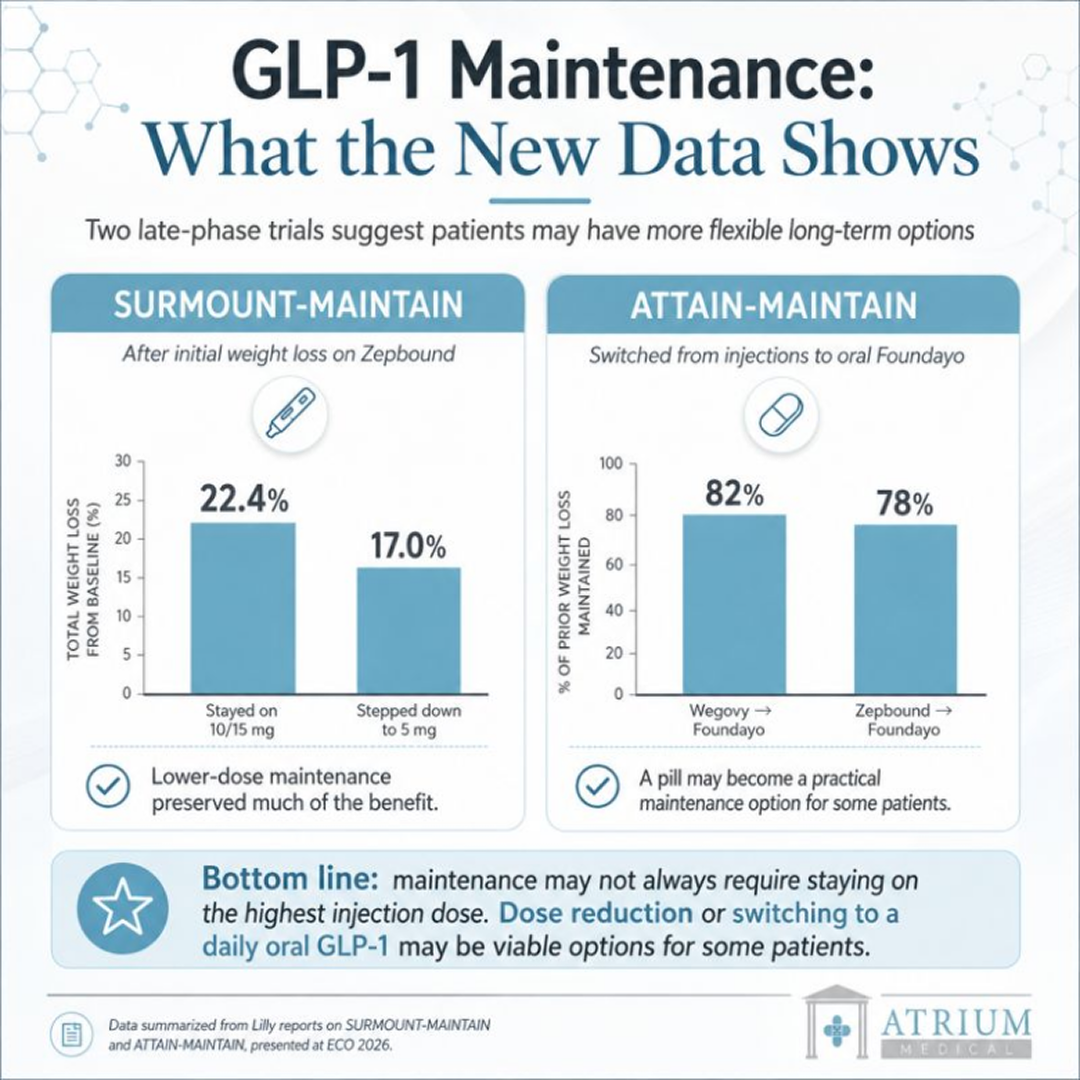
The most important new GLP-1 data is not only about how much weight people lose. It is about how much weight they can keep off.
In company-reported late-phase maintenance data, patients in SURMOUNT-MAINTAIN first lost weight on higher-dose Zepbound, then either continued the maximum tolerated dose or stepped down to 5 mg for a maintenance year. At week 112, the full-dose group remained down 22.4% from baseline, while the 5 mg group remained down 17.0%. Lower-dose therapy did not fully match continued high-dose therapy, but it preserved a large amount of the benefit.
The oral switch data is also important. In ATTAIN-MAINTAIN, patients who had plateaued after injectable therapy switched to oral orforglipron, marketed as Foundayo. After one year, patients switching from Wegovy maintained about 82% of their prior weight loss, while patients switching from Zepbound maintained about 78%.
That does not mean everyone should step down or switch to a pill. It means maintenance is becoming a real treatment phase, not an afterthought. For some patients, the right answer may be staying on the same dose. For others, it may be lowering the dose to reduce side effects, cost, or treatment burden. For some patients near goal weight, an oral maintenance option may eventually become attractive.
The bigger lesson is simple: obesity treatment is chronic care. The goal is not just losing weight. The goal is building a plan patients can actually stay on.
Insurance, prior authorization, and the 2026 Medicare GLP-1 Bridge Program
Coverage is one of the most frustrating parts of GLP-1 care. Diabetes indications and obesity indications are often treated differently by insurance plans. Many plans require prior authorization, BMI documentation, weight-related conditions, prior treatment history, and evidence of lifestyle efforts. Some employer plans still exclude weight loss medications entirely.
Atrium helps patients understand the process, but we cannot guarantee coverage. Medication cost is separate from the medical visit. The best approach is to assume coverage is uncertain until your plan is checked. Patients can also review accepted insurance plans before scheduling, but medication coverage is always plan-specific and often requires separate pharmacy-benefit review.
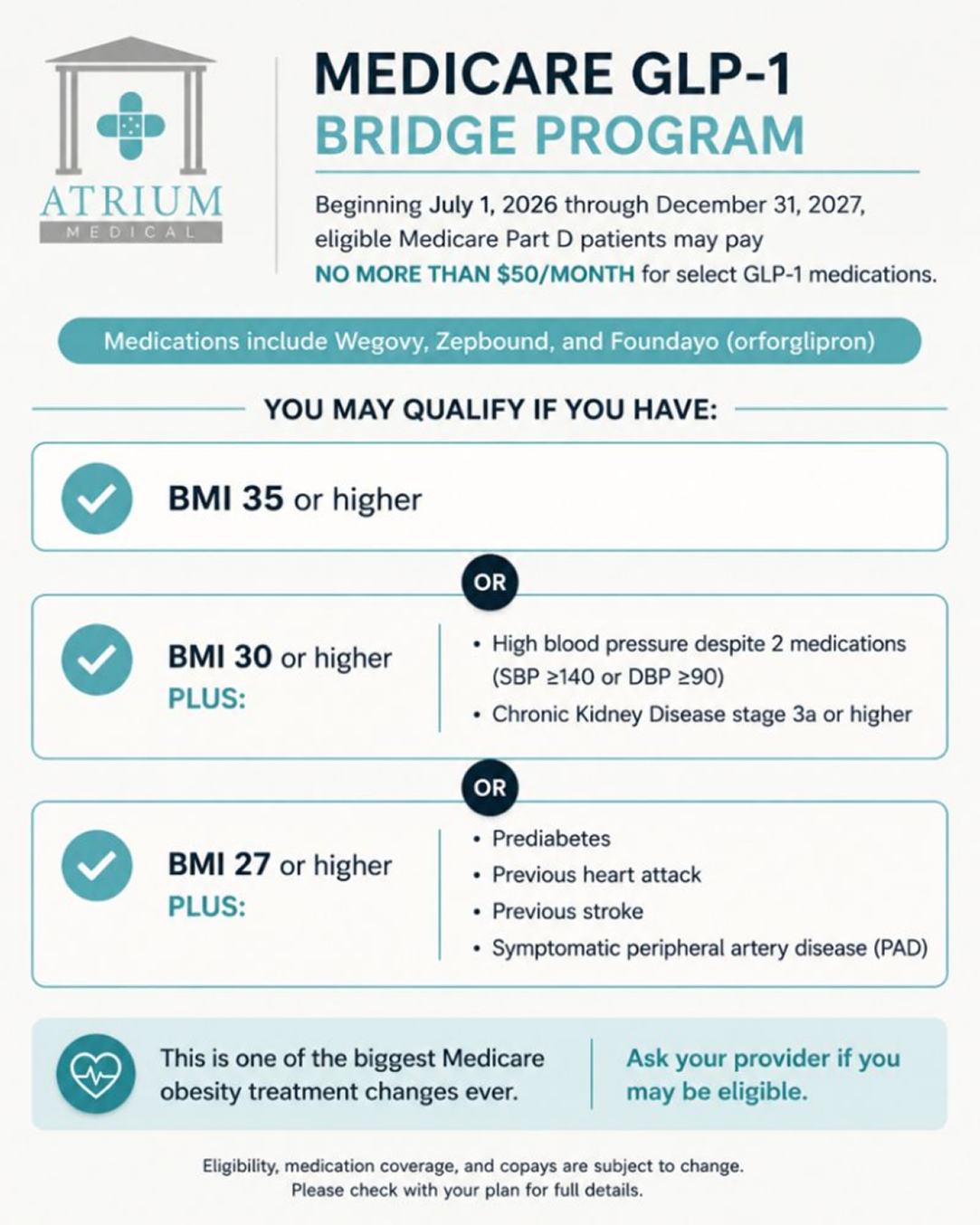
The 2026 Medicare GLP-1 Bridge Program Explained
A major policy change is now emerging for Medicare. Beginning July 1, 2026, the Medicare GLP-1 Bridge Program may allow eligible Medicare Part D patients to access certain obesity-indicated GLP-1 medications, including Foundayo, Wegovy, and certain Zepbound formulations, for no more than $50 per month through December 31, 2027. The important word is eligible. This is not universal GLP-1 coverage, and patients should not assume every medication, dose, plan, or diagnosis will qualify.
For NYC patients approaching Medicare or already enrolled in Part D, this may become an important bridge between today’s uneven obesity-drug coverage and broader future access. Atrium can help patients prepare by documenting BMI, weight-related conditions, prior treatment history, medication tolerance, labs, and the clinical reason a GLP-1 is being considered. We cannot guarantee approval, but clean documentation matters.
Compounded GLP-1s and online medication risk
Patients are seeing compounded semaglutide, compounded tirzepatide, gray-market peptides, and online offers everywhere. Some of this is driven by cost and access problems. Some of it is driven by marketing.
Compounded medications are not the same as FDA-approved branded products. There may be legitimate circumstances where compounding is discussed, but patients should understand sourcing, dosing, regulatory status, quality control, and safety risks before using any product advertised online.
To be clear: Atrium Medical does not sell unbranded gray-market injections, unverified house blends, research-use products, or medication mixes marketed as cheaper Ozempic, Wegovy, Mounjaro, or Zepbound substitutes. When compounding is discussed, the question is not only price. It is legality, pharmacy legitimacy, formulation, dosing, oversight, side effects, and whether an FDA-approved option is safer or more appropriate. We do not prescribe unverified compounded alternatives from online mills; we prioritize authentic, FDA-approved metabolic therapies
The FDA has warned about dosing errors and adverse events involving compounded injectable semaglutide products. This is exactly why medical supervision matters. A vial and syringe are not the same as a care plan.
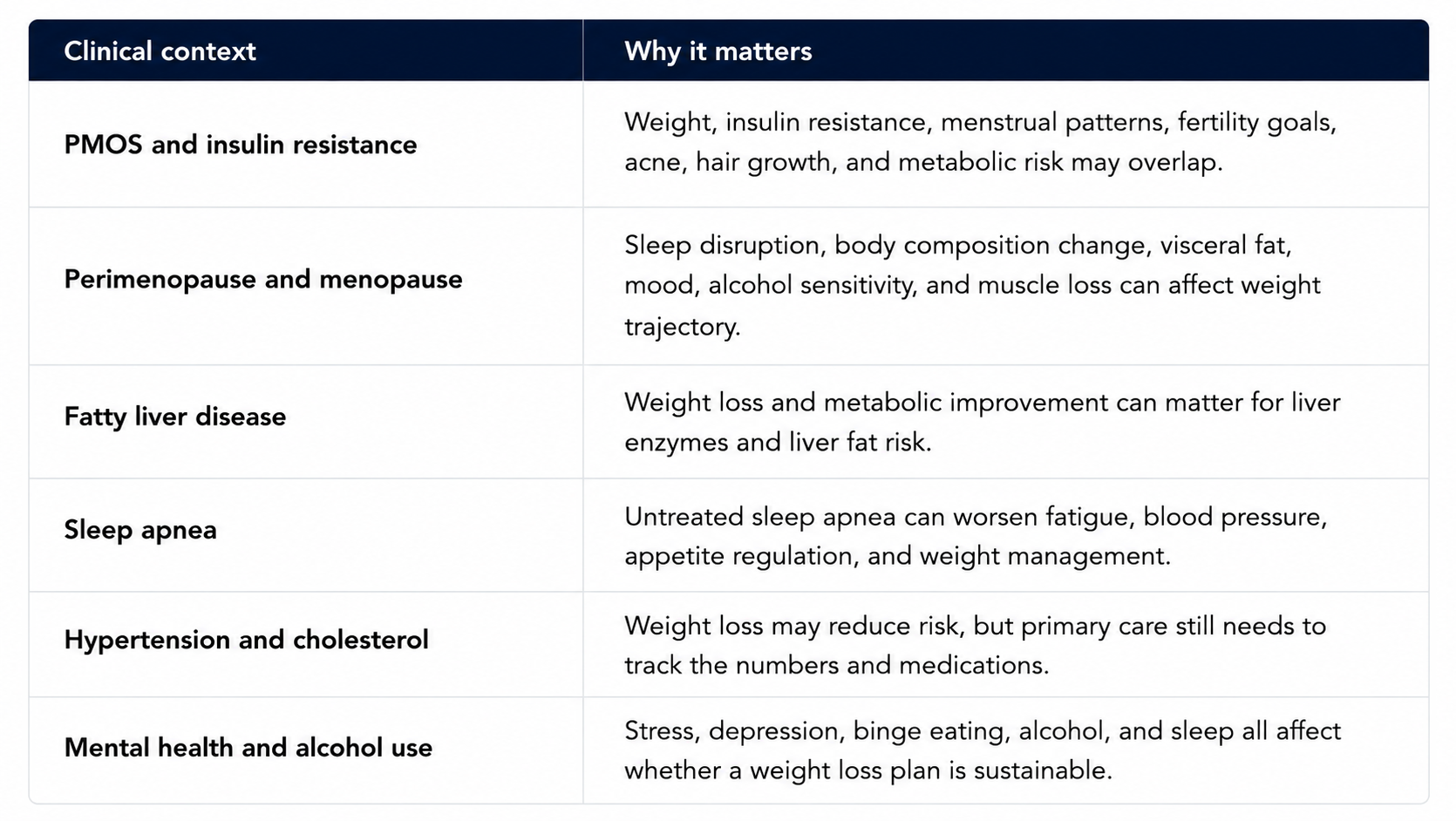
PMOS, menopause, fatty liver, sleep apnea, and cardiometabolic risk
Medical weight loss touches several areas that a primary care practice is already built to manage.
GLP-1 microdosing and dose manipulation
Patients ask about microdosing for multiple reasons, all of which are legitimate concerns:
Managing side effects. Nausea, constipation, and reflux are common, especially during dose escalation, and going slower or staying lower feels like the obvious fix.
Cost. Branded injectables can run over $500 a month without full coverage. Stretching a pen or using less per dose looks like an easy way to extend a prescription.
Maintenance. Patients near goal weight are often looking for a lower, steady dose rather than continued escalation, and do not see why they would need the full treatment dose forever.
Patients try to solve these three problems in multiple ways. Unfortunately, each one has a real, specific problem attached to it:
Counting clicks on a pen. Whether this is mechanically possible depends on the exact device and market. Ozempic is a dial-adjustable multidose pen. In the United States, FDA approved four-dose Mounjaro and Zepbound KwikPens on January 20, 2026, while single-dose Mounjaro and Zepbound pens and vials also remain in use. The KwikPens have a dose knob, but Lilly labels them as delivering four fixed doses and does not provide a validated click-to-milligram conversion for fractional dosing. Online click charts therefore describe an off-label workaround, not a manufacturer-approved dosing method. Wegovy single-dose pens do not have a click-counting mechanism. Atrium does not recommend patients improvise partial doses from any pen without direct prescribing supervision.
Sourcing a compounded low-dose vial. This is no longer the workaround it was two years ago. Both the semaglutide and tirzepatide shortages that made compounding legally available were declared resolved in 2024 and 2025, the compounding wind-down deadlines have passed, and in April 2026 the FDA proposed closing the remaining legal pathway entirely. Outside narrow, documented medical need, compounded versions of these drugs are no longer a lawful option, and FDA has logged hundreds of adverse event reports, some requiring hospitalization, tied to dosing errors from patients measuring their own doses out of compounded vials.
Stretching the interval, taking the lowest dose every other week instead of weekly. Semaglutide and tirzepatide are dosed weekly because their half-lives are built around a weekly schedule to maintain steadier blood levels. Stretching the interval has not been adequately studied and may create more variable exposure rather than the stable, tolerable dose the patient is trying to achieve.
Encouragingly, there may now be a better solution than any of these three “hacks.” Novo Nordisk’s Wegovy pill, an oral form of semaglutide, was FDA-approved in December 2025 and launched in January 2026. It is a studied medication with its own approved dosing schedule, not a workaround. Here is how it holds up against each reason patients consider microdosing:
For side effects: the pill is not automatically gentler. Trial data show comparable rates of nausea, vomiting, and diarrhea to the injectable. What it trades is a needle for a strict fasting-state routine: taken on an empty stomach with minimal water, followed by a 30-minute wait before eating, drinking, or taking other medication. For some patients that is easier to live with. For others, a once-weekly injection is simpler than a daily ritual.
For cost: this is the stronger case. Wegovy’s pill launched at a substantially lower cash price than the branded injectable. If cost is the actual driver, oral semaglutide is now a legitimate, FDA-approved answer rather than a compounded or device-manipulation workaround.
For maintenance: less clean. The pill has its own titration schedule, and there is no more evidence for inventing a below-label maintenance regimen with the tablet than with the injectable. Choosing oral treatment does not eliminate the need for an individualized, supervised dosing plan.
One limitation worth stating plainly: this option currently exists only for the semaglutide family. There is no FDA-approved oral tirzepatide. A patient on Zepbound or Mounjaro does not have this alternative yet.
Ozempic face: Is it real?
Many patients ask about “Ozempic face” because appearance is often part of the motivation for losing weight in the first place. The term describes facial hollowing, looser skin, deeper folds, and a more aged appearance that can become noticeable after substantial weight loss on semaglutide, tirzepatide, or another GLP-1 medication.
Weight loss is the main driver. The face contains distinct fat compartments in the temples, cheeks, under-eye area, and lower face. When weight falls quickly, those compartments lose volume faster than the overlying skin can fully retract. A 2025 radiographic study found an average 7% reduction in midfacial volume for every 10 kilograms of total weight lost, with most of the change occurring in superficial facial fat pads. Similar facial changes have long been observed after bariatric surgery and other forms of rapid, major weight loss, which is why “Ozempic face” is not unique to Ozempic.
The amount and speed of weight loss matter, but they are not the only variables. Age, genetics, baseline facial volume, skin elasticity, smoking history, sun damage, nutrition, and the degree of muscle loss all influence how visible the change becomes. Two patients can lose the same amount of weight and have very different facial outcomes.
There may also be a deeper biological layer, but this evidence is still emerging. Reviews have proposed that GLP-1 signaling, changes in adipose-derived stem cells, oxidative stress, and dermal remodeling could affect collagen support and skin architecture beyond the mechanical loss of facial fat. These mechanisms are scientifically plausible, but they are not yet established well enough to say that GLP-1 drugs directly age the face independent of weight loss.
The skin effects may also run in two directions at once. GLP-1 medications improve glucose control and reduce systemic inflammation, which may reduce glycation stress on collagen. Early studies and case reports suggest possible benefits in psoriasis, hidradenitis suppurativa, and wound healing. Those findings are promising but remain preliminary and are not established reasons to prescribe a GLP-1 solely for a skin condition.
What can patients do? There is no proven way to prevent facial fat loss while selectively losing fat elsewhere. The practical goal is to reduce avoidable contributors: titrate thoughtfully rather than racing to the highest dose, avoid unnecessarily rapid weight loss, prioritize adequate protein, perform resistance training to preserve lean tissue, and monitor for iron, zinc, vitamin D, vitamin B12, vitamin A, and other deficiencies when intake is substantially reduced. These steps support overall tissue health but cannot guarantee that facial volume will be preserved.
The bottom line is that “Ozempic face” is real, but the phrase oversimplifies the biology. The visible change is driven mainly by the magnitude and pace of weight loss. Possible direct effects on skin-supporting cells remain an emerging research question, while the same medications may simultaneously improve inflammatory and metabolic processes within the skin.
Buying GLP-1 medications online: what patients should know
Online access has made GLP-1 medications easier to obtain, but convenience and clinical oversight are not the same thing.
In a 2026 JAMA secret-shopper study, a slender Yale medical student posed as a 237-pound patient and attempted to obtain semaglutide or tirzepatide from 49 direct-to-consumer websites. Forty-five of the 49 sites prescribed a GLP-1 medication, including some that issued a prescription within five minutes.
The gaps in evaluation were striking:
- Almost two-thirds did not require a live conversation with a clinician.
- Roughly half did not ask about eating disorders.
- Nearly two-thirds did not require vital signs or laboratory information.
- More than four out of five did not ask whether the patient had a regular physician.
This does not mean telehealth is inherently unsafe. A well-run telehealth practice can provide thoughtful, appropriate medical care. The concern is whether the platform is actually evaluating the patient or simply moving the patient through a sales funnel.
A proper GLP-1 assessment may include weight history, prior treatment, medications, eating behavior, gastrointestinal symptoms, pregnancy plans, gallbladder or pancreatic history, kidney function, metabolic risk, contraindications, and a plan for side effects and follow-up.
Many online platforms also prescribe compounded semaglutide or tirzepatide. Compounded medications are not FDA-approved, and the FDA does not review them before sale for safety, effectiveness, potency, sterility, or manufacturing quality. The agency has reported dosing errors, products with fraudulent labels, and adverse events associated with compounded GLP-1 medications. FDA has also warned that poor compounding practices can create contamination or potency problems, although that concern applies to compounded drugs generally rather than proving that every compounded GLP-1 product is contaminated.
The practical question is not simply how quickly a prescription arrives. It is whether a qualified clinician obtained enough information to decide that the medication is appropriate, prescribed a reliable product, and remained available to manage what happens next.
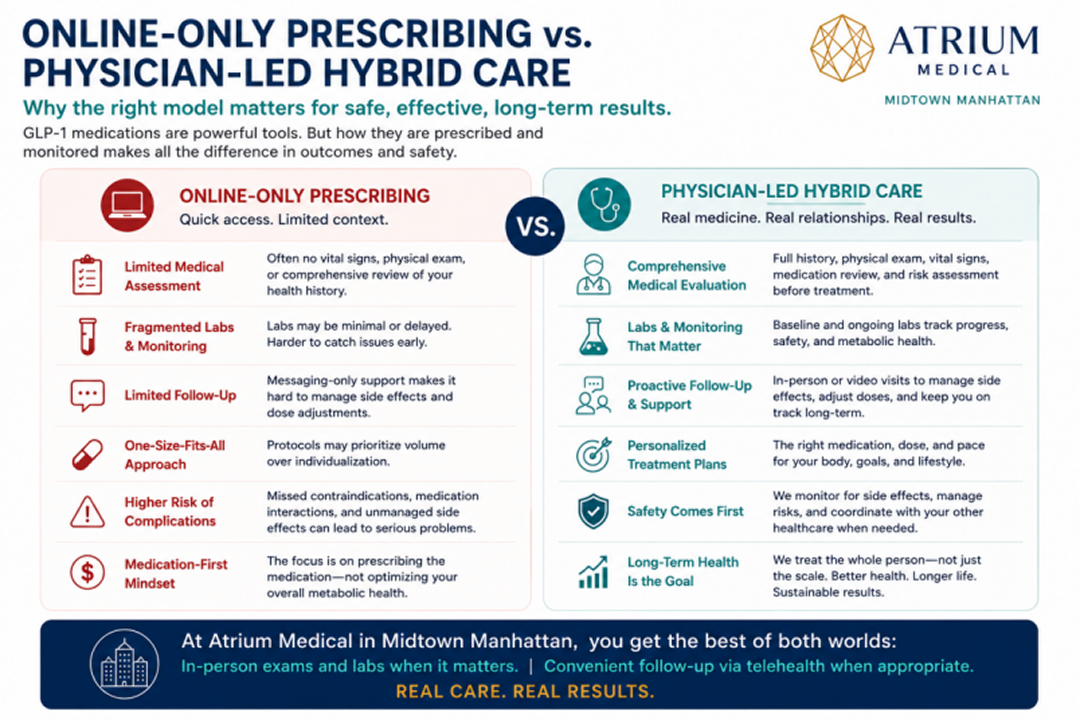
How Atrium manages GLP-1 care in Midtown Manhattan
Online-only care can prescribe. A real primary care practice can follow the whole patient.
At Atrium Medical, GLP-1 care can combine in-person evaluation, labs, vitals, side-effect assessment, insurance documentation, and televisit follow-up when appropriate. If the next step is labs, blood pressure review, abdominal symptoms, dehydration risk, an exam, or a medication adjustment, you are not stranded with a chat box.
Our office is located at 160 East 56th Street, 12th Floor, in Midtown Manhattan, close to the 59th Street subway hub, Grand Central, Park Avenue, Lexington Avenue, Bloomberg, JPMorgan, Sutton Place, Turtle Bay, Lenox Hill, and the broader Midtown East office corridor.
If you are new to the practice, the right starting point may be a new patient visit or an annual physical exam in NYC , depending on whether the priority is weight-loss medication evaluation, broader prevention, or ongoing independent primary care in NYC .
Medical Weight Loss FAQ
No. Some GLP-1 and related medications are approved for chronic weight management in eligible adults without diabetes. Other products are approved for type 2 diabetes. The indication, dose, insurance coverage, and medical appropriateness depend on the specific medication and patient.
Ozempic contains semaglutide and is approved for type 2 diabetes, while Wegovy contains semaglutide and is approved for chronic weight management. Patients often use the names interchangeably online, but the medical and insurance distinction matters.
Tirzepatide, marketed as Zepbound for weight management, has shown higher average weight loss than semaglutide in many trial comparisons. But the right medication depends on safety, side effects, coverage, dose tolerance, and the patient’s long-term plan.
Not as a routine prescription medication. Retatrutide is an investigational once-weekly triple agonist that targets GLP-1, GIP, and glucagon receptors. Lilly has reported strong Phase 3 results, including 28.3% average weight loss over 80 weeks at the highest studied dose in one obesity trial, but the drug still requires regulatory review. Patients should not inject research-use or online products marketed as retatrutide. Those products are not the same as a studied pharmaceutical product.
Yes. Oral options are emerging quickly, including oral semaglutide formulations and orforglipron, marketed as Foundayo. They may be useful for some patients, but they still require medical supervision.
For many patients, appetite signaling returns and weight regain is common after stopping . A maintenance strategy matters: nutrition, resistance training, follow-up, medication adjustment, dose reduction, switching, or continued therapy depending on the patient.
Not necessarily, but obesity is chronic for many patients. Some may remain on therapy. Some may lower dose. Some may switch medications. Some may stop and maintain with intensive behavioral and metabolic support. There is no one answer for everyone.
Weight loss can include lean mass, especially if calorie intake drops without adequate protein and resistance training. A good medical plan should protect muscle and function, not just reduce scale weight.
Compounded medications are not the same as FDA-approved branded products. Source, dose, formulation, quality, prescribing oversight, and regulatory status matter. Atrium Medical does not sell unverified gray-market injections, unbranded house blends, research-use products, or medication mixes marketed as cheaper substitutes for approved GLP-1 medications.
Coverage is highly plan-specific. Some plans cover obesity medications with prior authorization. Others exclude them. Diabetes indications are often treated differently from obesity indications. Atrium can help patients understand the documentation process, but coverage cannot be guaranteed.
Often, yes. Many follow-up visits, lab reviews, dose discussions, and side-effect check-ins can be handled by televisit when appropriate. In-person visits are still important when vitals, labs, exam, or safety issues need hands-on assessment
No. Atrium’s medical weight loss approach is focused on obesity, overweight with weight-related conditions, and metabolic health. We do not treat these medications as short-term cosmetic tools.
Microdosing is not an FDA-approved regimen and has not been validated in clinical trials. Whether partial dosing is mechanically possible depends on the exact device. Ozempic and the four-dose Mounjaro and Zepbound KwikPens have dose knobs, but the manufacturers do not provide validated click-to-milligram instructions for fractional dosing. Other presentations, including Wegovy single-dose pens and many Mounjaro or Zepbound single-dose devices, cannot be click-counted at all. Atrium does not recommend DIY dose manipulation. If cost, side effects, or maintenance dosing is the concern, dosing should be individualized with the prescribing clinician.
“Ozempic face” describes facial hollowing, looser skin, and deeper folds that can follow substantial weight loss on Ozempic or another GLP-1 medication. The main driver is loss of facial fat, especially when weight is lost rapidly. Age, baseline facial volume, skin elasticity, genetics, nutrition, and muscle loss also affect how visible the change becomes. There is no proven way to prevent facial fat loss selectively, but thoughtful dose escalation, avoiding unnecessarily rapid weight loss, adequate protein, resistance training, and correction of nutrient deficiencies may support healthier overall body composition and skin.
Medical sources and official references
- CDC: obesity overview
- FDA: concerns about unapproved GLP-1 drugs used for weight loss
- FDA: dosing errors associated with compounded injectable semaglutide
- FDA: Foundayo (orforglipron) approval announcement
- Reuters: Lilly retatrutide TRIUMPH-1 Phase 3 obesity data
- Lilly investor disclosure: retatrutide TRIUMPH-1 results
- PubMed: ATTAIN-MAINTAIN oral orforglipron maintenance data
- PubMed: weight regain after stopping GLP-1 therapy
- CMS: Medicare GLP-1 Bridge Program
- FDA: GLP-1 compounder enforcement and shortage resolution timeline
- Diabetes Care: microdosing semaglutide in multidose pens, Komé et al., 2025
- FDA approval letter: Mounjaro KwikPen, January 20, 2026
- FDA approval letter: Zepbound KwikPen, January 20, 2026
- Lilly: Zepbound KwikPen Instructions for Use
- JAMA: Online prescribing of GLP-1 receptor agonists, Chetty et al., 2026
- FDA: Concerns with unapproved and compounded GLP-1 drugs
- Radiographic midfacial volume changes in patients taking GLP-1 medications, 2025
- Systematic review: GLP-1 receptor agonists and dermatologic effects, 2025
- American Academy of Dermatology: How GLP-1 drugs can affect skin, hair, and nails
BOOK YOUR MEDICAL WEIGHT LOSS CONSULTATION AT ATRIUM MEDICAL
To schedule a medical weight loss consultation with Atrium Medical, call 212-457-1722 or book online. Our clinicians can help review your medical history, baseline labs, medication eligibility, insurance pathway, side-effect concerns, and long-term maintenance plan.





